Depression is an increasing health concern, affecting an estimated 280 million people worldwide.1 Alarming statistics indicate that over 30% of these cases fall under the category of treatment-resistant depression.2 Treatment-resistant depression typically refers to an “inadequate response to at least one antidepressant trial of adequate doses and duration,” a condition that imposes a significant burden on individuals, families, healthcare systems, and society at large.3
Fortunately, Transcranial Magnetic Stimulation (TMS), a non-invasive brain stimulation technique, offers hope for those diagnosed with treatment-resistant depression. Depression has always been considered a chronic lifelong illness. More than 50% of individuals who have had depression experience recurrent depressive episodes following initial symptom remission. Even after a traditional course of medication, a recurrence of four to five major depressive episodes is considered typical. Studies have shown that approximately 50-60% of individuals with treatment-resistant depression experience clinically significant improvements after TMS treatment.4 Additionally, an encouraging one-third achieve complete remission. Therefore, TMS’s ability to decrease the likelihood of recurrence makes it a particularly remarkable advancement.5
What is Transcranial Magnetic Stimulation?
Transcranial Magnetic Stimulation (TMS) is a non-invasive technique that utilizes electromagnetic induction to stimulate the brain with precise magnetic impulses. Electromagnetic induction is the process by which alterations in a magnetic field lead to the generation of electric currents, and conversely, changes in electric currents also produce a magnetic field. By generating magnetic fields, TMS may influence neuronal activity in specific brain regions, thereby altering cognition and behavior.
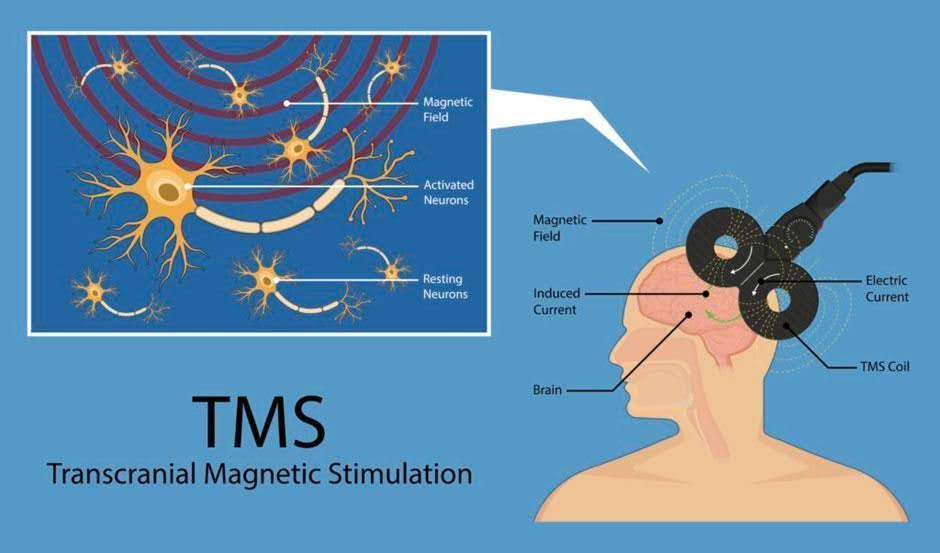
The way magnetic fields affect an individual’s brain is related to the pulse frequency produced by the TMS instrument. Pulse refers to the cycles of turning the magnetic fields on and off, and the frequency is determined by the number of pulses per second, measured in Hertz (Hz). Low frequency stimulation (< 1 Hertz) has an inhibitory effect, and high frequency stimulation (> 1 Hertz) has an excitatory effect on the brain. An inhibitory TMS results in a decrease in neuron activity, while an excitatory TMS results in an increase in neuron activity. Low frequency inhibitory TMS has shown a significant efficacy in treating positive symptoms of schizophrenia, such as auditory hallucinations.6 On the other hand, high-frequency excitatory TMS often produces a reduction in depression symptoms in clinical practice.
What Happens to the Depressed Brain?
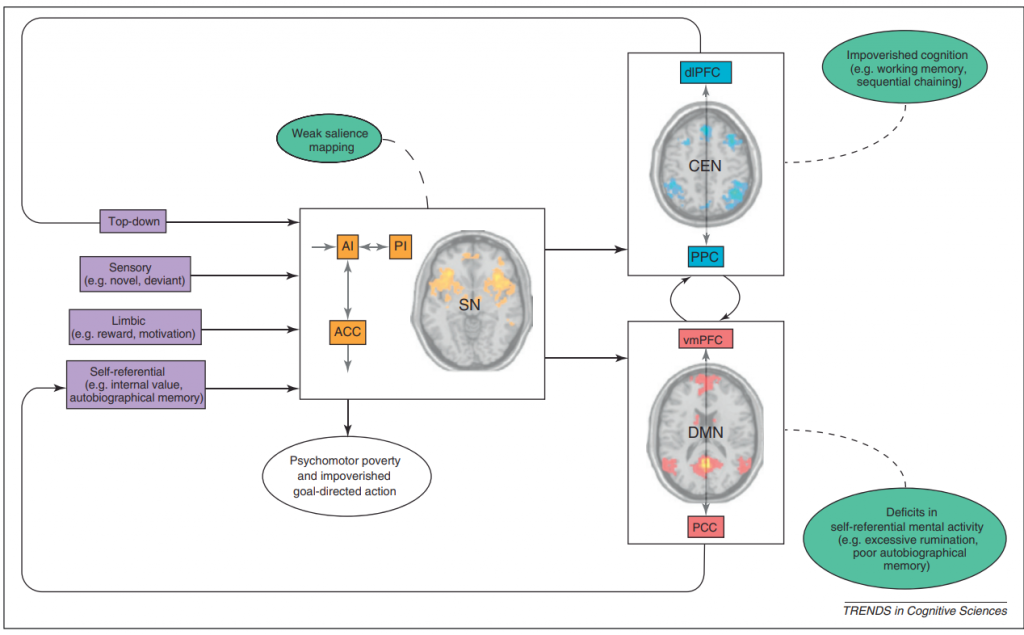
The most characteristic features of depression include ruminating on automatic negative thoughts. Rumination involves repetitive thinking regarding negative feelings and distress. An increased and dysregulated functional connectivity within the brain’s Default Mode Network (DMN) is responsible for self-referential processing and repetitive negative thinking, including ruminative brooding.7 At the same time, the Central Executive Network (CEN), the voluntary attention network, which is responsible for cognitive control, is under-active in depression. This hypoactivity in the CEN likely contributes to challenges regulating attention and concentration among people who are depressed, making it harder to break free from negative thought patterns.
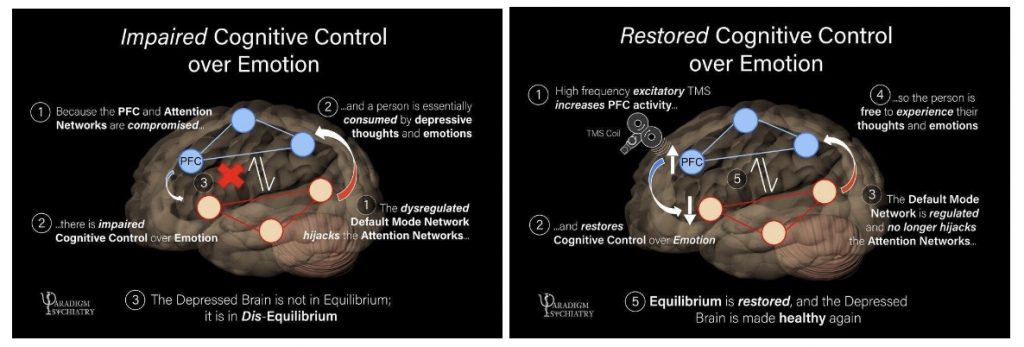
When combined, the hyperactivity of DMN and the hypoactivity of CEN puts the brain in disequilibrium, resulting in impaired cognitive control over attention and emotion.
In What Ways Does TMS Alleviate Depression?
Research has found a functional asymmetry of the Dorsolateral Prefrontal Cortex (DLPFC), a substructure of the CEN, in patients with depression. The DLPFC plays a central role in executive control in our brain, such as switching attention, working memory, and inhibition. Nonetheless, individuals with depression have hypoactivation in the left hemisphere of the DLPFC and hyperactivation in the right hemisphere of the DLPFC. The clinical effects of TMS are thus putatively linked to “re-balancing” activity between these two hemispheres within the CEN.8 By inducing high-frequency excitatory TMS to the left DLPFC, the activity in the left hemisphere may be increased, thereby potentially balancing altered brain activity associated with depression. Consequently, this neurostimulation also modulates the CEN and may restore cognitive control over attention and emotion.
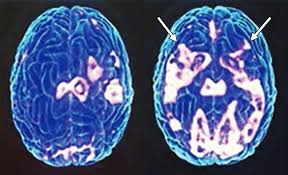
Besides this functional imbalance, brain imaging further suggests a structural hemispheric imbalance in individuals with depression. Studies have specifically found decreased fractional anisotropy in the left middle frontal gyrus before treatment in individuals with depression.9, 10 After TMS, researchers discovered increased fractional anisotropy, which is indicative of an improvement in depressive symptoms.9
Functional Connectivity: Impact beyond DLPFC
TMS applied to the left DLPFC improves both the functional and structural imbalance of the two hemispheres, and increases activity of the CEN, which DLPFC is involved in. However, it is important to keep in mind that brain regions coordinate through many connected circuits and networks, which interact with each other.
In addition to improving the structural and functional integrity of the CEN, it is crucial to consider the attention network when treating depression. The attention network is primarily separated into the CEN and the Salience Network.
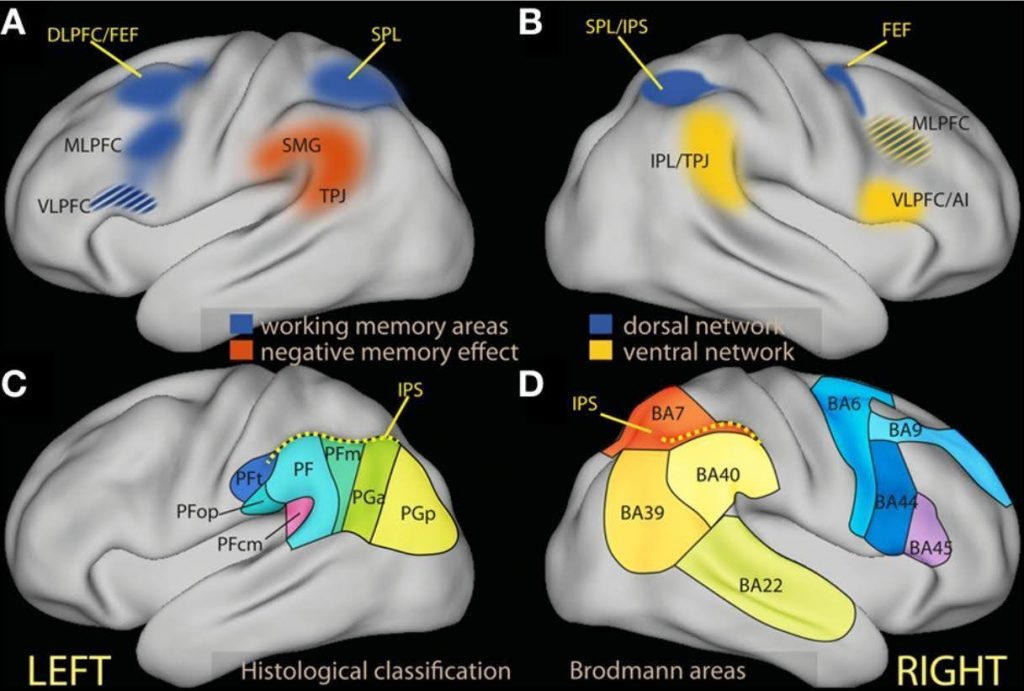
The CEN generally involves a “top-down” selection of stimuli and responses, which requires voluntary cognitive control. The network includes dorsal frontal areas such as DLPFC and the superior parietal lobule.4,11 It is responsible for maintaining attention in the face of distraction, voluntary orienting in spatial attention and stimulus selection. For example, core symptoms of depression include attention impairment, such as top-down selective attention (“I only want to see sad things”), difficulty disengaging from the negative stimuli (“I cannot stop looking at sad things”), and the inability to sustain focus.
Unlike the CEN, the salience network is responsible for the “bottom-up” detection of stimuli, which means that the network automatically picks up unexpected information that it detects without conscious effort. Core regions include the inferior parietal lobule and the temporoparietal junction.11, 12 Research has also found that salience network activity implicates memory, particularly self-relevant emotional experiences, showing its importance in emotional and attentional function.11 For example, individuals with depressive symptoms often present a bottom-up negative attentional bias (“My attention draws to negative things before I notice it consciously”), which is related to the maintenance and recurrence of depressive episodes.
In short, the CEN essentially enables “top-down” attentional control for maintaining attention and stimuli selection, while the SN is necessary for “bottom-up” responding to unexpected and/or emotionally-salient stimuli.
How Does TMS Improve Connectivity Dysfunction in Depression?
Although all networks are functionally specialized, they should be considered as a whole rather than distinct because the coordination and interaction between the two networks are essential for effective control over attention, cognition, and behavior. For example, in the context of depression, there is reduced functional connectivity in the CEN between the temporoparietal junction and the DLPFC.13 Moreover, TMS application to the left superior parietal lobule produces a significant enhancement in processing speed and resting-state connectivity of the CEN in healthy subjects.14 Additionally, research shows that applying TMS to the left DLPFC can decrease the functional connectivity between the DLPFC and DMN areas in patients with depression, which potentially reduces rumination and improves depressive symptoms.10
Furthermore, increasing functional connectivity in the DMN and CEN networks might also collectively improve sustained and transient top-down attentional control, which may help address one of the symptoms of depression, trouble concentrating or focusing.11 This improvement in connectivity facilitates more efficient communication between neural networks involved in attention.
TMS Modulates the Brain as a Whole
Overall, the application of TMS represents a significant advancement in the treatment of depression, offering renewed hope and a path towards improved mental health for those who have struggled with treatment-resistant forms of this debilitating condition. However, further research and clinical trials are necessary to investigate the relationship between TMS and these networks before its widespread implementation. For example, there is little research investigating SN in depression with TMS, although there exists a significantly reduced connectivity within this circuit. Although much remains to be investigated, current findings are promising — through the targeted and non-invasive approach of TMS, clinicians may be able to address both structural and functional imbalances in the depressed brain, paving the way for a more comprehensive and effective approach to depression treatment.
Acknowledgements
I would like to express my deepest gratitude for J.D.Allen, Ph.D., a visiting scholar in the Department of Psychology in University of California, Berkeley, for so generously reviewing my article and providing detailed and thorough feedback for my work.
References
- GBD results. (n.d.). Institute for Health Metrics and Evaluation. https://vizhub.healthdata.org/gbd-results/
- Zhdanava, M., Pilon, D., Ghelerter, I., Chow, W., Joshi, K., Lefèbvre, P., & Sheehan, J. J. (2021). The prevalence and National Burden of Treatment-Resistant Depression and Major Depressive Disorder in the United States. The Journal of Clinical Psychiatry, 82(2). https://doi.org/10.4088/jcp.20m13699
- Fava, M. (2003). Diagnosis and definition of treatment-resistant depression. Biological Psychiatry, 53(8), 649–659. https://doi.org/10.1016/s0006-3223(03)00231-2
- Stern, A. P., MD. (2020). Transcranial magnetic stimulation (TMS): Hope for stubborn depression. Harvard Health. https://www.health.harvard.edu/blog/transcranial-magnetic-stimulation-for-depression-2018022313335#:~:text=Does%20TMS%20work%3F,their%20symptoms%20go%20away%20completely.
- Penner, J., Osuch, E. A., Schaefer, B., Théberge, J., Neufeld, R. W. J., Menon, R. S., Rajakumar, N., & Williamson, P. C. (2018). Temporoparietal junction functional connectivity in early schizophrenia and major depressive disorder. Chronic Stress, 2, 247054701881523. https://doi.org/10.1177/2470547018815232
- Cole, J. C., Green Bernacki, C., Helmer, A., Pinninti, N., & O’reardon, J. P. (2015). Efficacy of Transcranial Magnetic Stimulation (TMS) in the Treatment of Schizophrenia: A Review of the Literature to Date. Innovations in clinical neuroscience, 12(7-8), 12–19.
- Antičević, A., Cole, M. W., Murray, J. D., Corlett, P. R., Wang, X. J., & Krystal, J. H. (2012). The role of default network deactivation in cognition and disease. Trends in Cognitive Sciences, 16(12), 584–592. https://doi.org/10.1016/j.tics.2012.10.008
- Liu, W., Mao, Y., Wei, D., Yang, J., Du, X., Xie, P., & Qiu, J. (2016). Structural Asymmetry of Dorsolateral Prefrontal Cortex Correlates with Depressive Symptoms: Evidence from Healthy Individuals and Patients with Major Depressive Disorder. Neuroscience Bulletin, 32(3), 217–226. https://doi.org/10.1007/s12264-016-0025-x
- Peng H, Zheng H, Li L, Liu J, Zhang Y, Shan B, Zhang L, Yin Y, Liu J, Li W, Zhou J, Li Z, Yang H and Zhang Z (2012) High-frequency rTMS treatment increases white matter FA in the left middle frontal gyrus in young patients with treatment-resistant depression. Journal of Affective Disorders 136, 249–257.
- Schiena G, Franco G, Boscutti A, Delvecchio G, Maggioni E, Brambilla P (2021). Connectivity changes in major depressive disorder after rTMS: a review of functional and structural connectivity data. Epidemiology and Psychiatric Sciences 30, e59, 1–13. https://doi.org/10.1017/ S2045796021000482
- Viviani, R. (2013). Emotion regulation, attention to emotion, and the ventral attentional network. Frontiers in Human Neuroscience, 7. https://doi.org/10.3389/fnhum.2013.00746
- Vossel, S., Geng, J. J., & Fink, G. R. (2013). Dorsal and ventral attention systems. The Neuroscientist, 20(2), 150–159. https://doi.org/10.1177/1073858413494269
- Keller, A. S., Leikauf, J., Holt-Gosselin, B., Staveland, B. R., & Williams, L. M. (2019). Paying attention to attention in depression. Translational Psychiatry, 9(1). https://doi.org/10.1038/s41398-019-0616-1
- Anderková, Ľ., Pizem, D., Klobušiaková, P., Gajdoš, M., Koriťáková, E., & Rektorová, I. (2018). Theta burst stimulation enhances connectivity of the dorsal attention network in young healthy subjects: an exploratory study. Neural Plasticity, 2018, 1–6. https://doi.org/10.1155/2018/3106918
Image References
Figure 1: Tobietaca. (2022). What is TMS – TMS Therapy – Restore Brain. TMS Therapy – Restore Brain. https://restore-brain.com/tms-therapy-dallas/what-is-tms/
Figure 2: Jagtap, P. M., MD. (2021). How Does TMS relieve Depression? — Paradigm Psychiatry. Paradigm Psychiatry. https://paradigm-psychiatry.com/communityblog/how-does-tms-relieve-depression
Figure 3: Huntley, J. H., Habibabadi, R. R., Vaishnavi, S., Khoshpouri, P., Kraut, M. A., & Yousem, D. M. (2023). Transcranial Magnetic Stimulation and its Imaging Features in Patients With Depression, Post-traumatic Stress Disorder, and Traumatic Brain Injury. Academic Radiology, 30(1), 103–112. https://doi.org/10.1016/j.acra.2022.03.016
Figure 4: Viviani, R. (2013). Emotion regulation, attention to emotion, and the ventral attentional network. Frontiers in Human Neuroscience, 7. https://doi.org/10.3389/fnhum.2013.00746
Figure 5: Menon V. (2011). Large-scale brain networks and psychopathology: a unifying triple network model. Trends in cognitive sciences, 15(10), 483–506. https://doi.org/10.1016/j.tics.2011.08.003